
 Joachim Zuther, Lymphedema Specialist.
Joachim Zuther, Lymphedema Specialist.
“After a day of sitting in the office my ankles are swollen.”
“During the last several months of my pregnancy, my legs practically doubled in size”
“My fingers and hand frequently get puffy following a long hike”
“My arm started swelling after I had surgery for my breast cancer”
“Following the removal of a malignant lesion on my thigh, my leg started to get bigger”
“When I got stung by a bee on my cheek, I had a big swelling covering the entire side of my face”
Does any of this sound familiar? In some of these cases the term “swelling” can be interchangeably used with edema, in other cases the swelling must be considered as lymphedema. While the initial causes for the formation of the swelling in the above instances are different, all involve the accumulation of fluid in the soft tissues of the skin due to an insufficiency of the lymphatic system.
A physician with knowledge of lymphedema is able to easily establish the diagnosis of lymphedema by taking the patients medical history and performing a physical examination. This includes measuring the circumference of the affected arms or legs to determine the severity of fluid buildup in affected limbs. The physician determines whether symptoms, such as swelling in the arms or legs, might be caused by other conditions, including blood clots, or cardiac insufficiencies, which are treated differently. To further establish the diagnosis, certain imaging tests may be performed in order to conclude the exact cause of the fluid buildup in the tissues.
These tests may include:
- Lymphscintiography (most commonly performed and considered to be the gold standard)
- Bioimpedance Spectroscopy (BIS)
- ICG Lymphography (Indocyanine Green), sometimes referred to as Fluoroscopy
- MRI
- CT
- Indirect Lymphography (not commonly performed in the US)
- others
You can also perform a self-check for Lymphedema before you make an appointment with a physician – take a personal assessment by answering the following questions:
- Is the swelling limited to one arm or leg?
- Did you have surgery or radiation prior to the onset of the swelling?
- Did you have an injury on your affected body part?
- Is the back of the hand/foot included in the swelling?
- Are the natural skin folds (elbow/knee, ankle/wrist) on your extremity deepened?
If the answer to some or all the above questions is “yes”, lymphedema may be present.
You can also perform the “Stemmer” Test by trying to lift a skin fold on the back of the second toe or middle finger.
If you are able to gently pinch and lift the skin fold, the Stemmer Sign is negative. If it is not possible to gently pinch and lift the fold, this may be an indication of tissue build-up as a result of protein accumulation in these tissues. In this case, the Stemmer Sign is positive and serves as an indication that lymphedema may be present. Please see below to learn about the treatment of lymphedema.
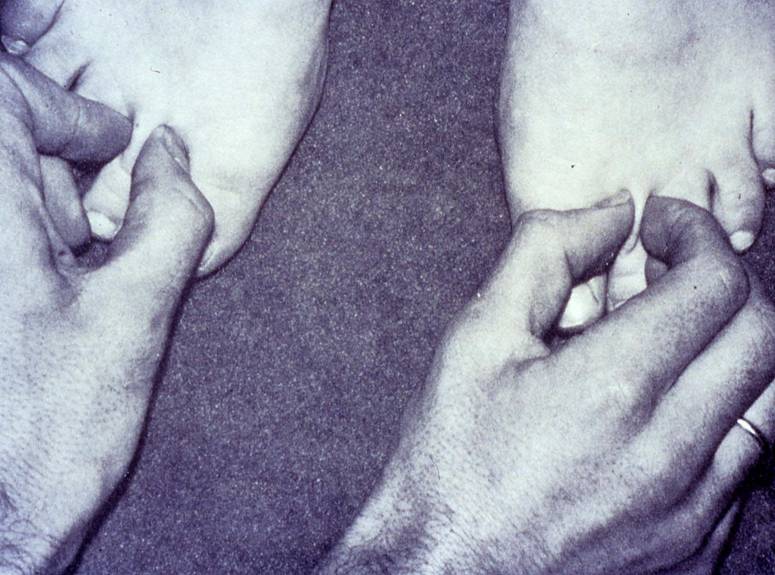
Stemmer sign positive on left (right leg)
Click here to view a video explaining the physicians diagnosis of lymphedema
The question is – when is a swelling considered edema, and when is it lymphedema?
In order to understand the differences, it is important to consider that a large portion of the human body consists of water. According to Guyton’s  Textbook of Medical Physiology, the water content of an average weight male is about 60%, in a female about 55%; in a male weighing 160 pounds, this amounts to approximately 40 liters (about 10.5 gallons) of water. About two thirds of the water resides inside the body’s cells in the intracellular fluid compartment, one third is located outside the cells in the extracellular compartment. Of the fluid residing outside the cells, one fifth is located inside blood vessels as intravascular fluid. The remaining fluid (approximately 10.5 liters) is distributed in the interstitial tissue between the cells (interstitial fluid).
Textbook of Medical Physiology, the water content of an average weight male is about 60%, in a female about 55%; in a male weighing 160 pounds, this amounts to approximately 40 liters (about 10.5 gallons) of water. About two thirds of the water resides inside the body’s cells in the intracellular fluid compartment, one third is located outside the cells in the extracellular compartment. Of the fluid residing outside the cells, one fifth is located inside blood vessels as intravascular fluid. The remaining fluid (approximately 10.5 liters) is distributed in the interstitial tissue between the cells (interstitial fluid).
 Fluids, gases (oxygen and carbon dioxide), nutrients and waste products are constantly exchanged between the blood and the interstitial tissue. The primary sites of this exchange are the blood capillaries, which are the smallest blood vessels and part of the body’s microcirculation. Blood capillaries have very thin walls, consisting of only one layer of cells. Gaps between these cells enable the exchange of these substances from the blood capillaries into the tissues and back. The water located in the interstitial tissue spaces is fluid that has leaked out of blood capillaries.
Fluids, gases (oxygen and carbon dioxide), nutrients and waste products are constantly exchanged between the blood and the interstitial tissue. The primary sites of this exchange are the blood capillaries, which are the smallest blood vessels and part of the body’s microcirculation. Blood capillaries have very thin walls, consisting of only one layer of cells. Gaps between these cells enable the exchange of these substances from the blood capillaries into the tissues and back. The water located in the interstitial tissue spaces is fluid that has leaked out of blood capillaries.
Edema occurs when excess levels of interstitial fluid accumulate, i.e., either too much water leaves the blood capillaries, or the water located in the tissues is not reabsorbed efficiently enough back into the blood capillaries. Edema may affect the entire body (anasarca, or generalized edema), or only certain parts of the body (localized edema).
In order to understand any swelling, the various factors and components involved in moving fluids throughout the body, and in and out of blood vessels need to be considered. The main components involved in this process are the cardiovascular system (heart and blood vessels) and the lymphatic system.
The cardiovascular system consists of an elaborate network designed to deliver oxygen and nutrients to body organs and to remove waste products  of metabolism from the tissues. Blood that has been oxygenated in the lungs is pumped out of the heart through the aorta, the largest artery in the body. The aorta arches upward from the left ventricle of the heart to the upper chest, and then travels down towards the abdomen forming the main trunk of the arterial circulation. The aorta then branches off into numerous smaller arteries, which deliver oxygen-rich blood to the various body systems. These arteries further subdivide into smaller vessels, and ultimately into blood capillaries, which consist of an arterial and a venous loop. The exchange of fluids, gases, nutrients and waste products between blood and tissue occurs across their walls.
of metabolism from the tissues. Blood that has been oxygenated in the lungs is pumped out of the heart through the aorta, the largest artery in the body. The aorta arches upward from the left ventricle of the heart to the upper chest, and then travels down towards the abdomen forming the main trunk of the arterial circulation. The aorta then branches off into numerous smaller arteries, which deliver oxygen-rich blood to the various body systems. These arteries further subdivide into smaller vessels, and ultimately into blood capillaries, which consist of an arterial and a venous loop. The exchange of fluids, gases, nutrients and waste products between blood and tissue occurs across their walls.
On its way back to the heart, the venous blood passes through progressively larger veins and ultimately connects with the heart. A large part of the waste products is extracted from the blood as it flows through the kidneys.
The lymphatic system consists of lymph nodes and a network of channels in the body that carry lymph fluid, which is a colorless fluid containing mainly  water, protein and white blood cells. The water content in the lymph fluid is comprised by a fraction of the fluid, which leaves the blood capillaries, but is not reabsorbed back into the blood capillaries. The lymphatic system runs parallel to the blood circulatory system and represents an accessory route for fluid to flow from the tissue spaces back to the bloodstream. The lymph fluid is returned to the blood circulation via larger lymphatic vessels (lymphatic trunks) and amounts to approximately 2-3 liters per day. Unlike the circulatory system, in which the heart acts as a pump to circulate blood, the lymphatic system does not have a pump to circulate lymph fluid. Instead, larger lymph vessels contain small muscles (lymph angions) within their walls, which contract consecutive sections of the lymph vessels to facilitate the movement of lymph through its vessels via a peristaltic effect.
water, protein and white blood cells. The water content in the lymph fluid is comprised by a fraction of the fluid, which leaves the blood capillaries, but is not reabsorbed back into the blood capillaries. The lymphatic system runs parallel to the blood circulatory system and represents an accessory route for fluid to flow from the tissue spaces back to the bloodstream. The lymph fluid is returned to the blood circulation via larger lymphatic vessels (lymphatic trunks) and amounts to approximately 2-3 liters per day. Unlike the circulatory system, in which the heart acts as a pump to circulate blood, the lymphatic system does not have a pump to circulate lymph fluid. Instead, larger lymph vessels contain small muscles (lymph angions) within their walls, which contract consecutive sections of the lymph vessels to facilitate the movement of lymph through its vessels via a peristaltic effect.
Under normal conditions the body thrives to maintain a balance of fluid in the tissues by ensuring that about the same amount of water entering the body also leaves it. However, a number of factors can upset the fluid balance in the body, which may cause the onset of edema or lymphedema.
Edema
Rather than a disease in itself, edema is a symptom that can be caused by a number of conditions, including:
- Congestive heart failure (CHF),
- Chronic venous insufficiency (CVI),
- Immobility (prolonged standing or sitting, paralysis)
- Pregnancy, or
- Pressure from tight jewelry, tight bandages or compression garments
In all these cases the accumulation of fluid in the interstitial tissues is caused by insufficient return of venous blood, or venous pooling. The high volume of blood and the consequent increase in hydrostatic pressure inside the veins and blood capillaries makes it difficult for fluid to move from the tissues back into the vessels. While the lymphatic system tries to correct this imbalance by working harder, the elevated levels of tissue fluid is too high for the lymph vessels to compensate.
Edema may also be caused by change in the concentration of serum proteins (hypoproteinemia). Proteins in the blood have the ability to retain some water and salts within the blood, and a lower level of proteins may affect the movement of fluid in and out of blood capillaries causing excess levels of water to accumulate in the tissues. A loss of serum proteins may be caused by kidney, liver or thyroid diseases, malnutrition, excessive bleeding, chronic draining wounds and excessive burns.
Inflammatory reactions caused by traumatic events and arthritis are also a common cause for the onset of edema.
 Edema is a visible and palpable accumulation of excess levels of fluid within the tissues. Gentle, steady pressure with a thumb on the edematous tissues produces a temporary indentation (pitting edema). Edema can be a transitory or permanent symptom and its treatment focuses on the correction of the underlying condition; if this condition can be resolved the edema dissipates. If the underlying cause can’t be corrected, edema may be treated by elevation of the affected body part, wearing compression garments, the administration of diuretics, or dietary changes focusing on a low salt intake.
Edema is a visible and palpable accumulation of excess levels of fluid within the tissues. Gentle, steady pressure with a thumb on the edematous tissues produces a temporary indentation (pitting edema). Edema can be a transitory or permanent symptom and its treatment focuses on the correction of the underlying condition; if this condition can be resolved the edema dissipates. If the underlying cause can’t be corrected, edema may be treated by elevation of the affected body part, wearing compression garments, the administration of diuretics, or dietary changes focusing on a low salt intake.
Lymphedema
Lymphedema results from the inability of the lymphatic system to perform one of its basic functions, the removal of water and protein from the tissues of a certain portion of the body. This insufficiency can be caused by  developmental abnormalities of the lymphatic system (primary lymphedema), or damage to the lymphatic system such as the removal or radiation of lymph nodes in cancer surgery, or infection of the lymphatic system (secondary lymphedema). Lymphedema can present in the extremities, head and neck, breast and trunk, or external genitalia. The accumulation of protein and water in the tissues may be gradual in some patients and sudden in others, the result is always a high-protein edema. The high protein content in lymphedema can lead to secondary complications, such as hardening of the tissues over time, infections and increase in volume, especially in untreated or mistreated lymphedema.
developmental abnormalities of the lymphatic system (primary lymphedema), or damage to the lymphatic system such as the removal or radiation of lymph nodes in cancer surgery, or infection of the lymphatic system (secondary lymphedema). Lymphedema can present in the extremities, head and neck, breast and trunk, or external genitalia. The accumulation of protein and water in the tissues may be gradual in some patients and sudden in others, the result is always a high-protein edema. The high protein content in lymphedema can lead to secondary complications, such as hardening of the tissues over time, infections and increase in volume, especially in untreated or mistreated lymphedema.
Contrary to edema, a low-protein swelling, lymphedema is a disease rather than a symptom and its underlying cause, the insufficiency of parts of the lymphatic system cannot be reversed. Lymphedema does not dissipate by itself and continues to progress without adequate treatment.
Treatment of Lymphedema
The goal of lymphedema management is to reduce the lymphedematous swelling to a normal or near normal size utilizing remaining healthy lymph vessels and other lymphatic pathways. Once the lymphedema is decongested, the secondary goal is to maintain the reduction and to prevent the reaccumulation of lymph fluid. These goals can be achieved with the internationally recognized “gold standard” of lymphedema treatment known as Complete (or Combined) Decongestive Therapy (CDT). CDT is recognized as the therapy of choice for lymphedema by the International Society of Lymphology (ISL), the National Lymphedema Network (NLN), the Lymphology Association of North America (LANA), the American Lymphedema Framework Project (ALFP), and the North American Lymphedema Education Association (NALEA).
CDT is a combination of manual lymph drainage (MLD), a gentle manual treatment technique designed to reroute stagnated lymph fluid, skin care, compression therapy (short-stretch bandages and compression garments), and decongestive exercises.
CDT should only be performed by properly trained therapists. Lymphedema therapists can be physical therapists and their assistants, occupational therapists and their assistants, physicians, nurses, chiropractors or massage therapists who have undergone specialized training in Complete Decongestive Therapy. Several schools in the United States educate and certify therapists in proper lymphedema management; these schools meet the training standards outlined by the Lymphology Association of North America (LANA).
Pharmaceutical options in the treatment of lymphedema are limited to antibiotics, which are used to prevent and treat infections commonly associated with lymphedema. Diuretics are generally harmful and may contribute to the worsening of lymphedema related symptoms if used long-term.
Intermittent pneumatic compression devices (IPC) may be indicated in suitable cases, but should always be used in combination with CDT and never as a sole mode of treatment.
Dear Lymphedema Blog Reader – if you like the contents on this website, please help to keep it going. A great amount of work and research is necessary to provide you with up-to-date information on this site. Your donation supports these efforts and associated administrative costs. Surplus funds will be donated to Lymphedema/Lipedema-related charitable endeavors. Please donate using the “Donate Now” button on the right upper hand of this page – Thank You!
Join Lymphedema Guru, a Facebook page solely dedicated to inform about all things related to lymphedema – news, support groups, treatment centers, and much more


Great article. It’s pretty complete for its size, with some material that I have not previously seen. I do have a question about an area that I’ve never seen much coverage is regarding the impact of infection. Any idea where I can find more on that topic. What I’m curious about is how infection reduces lymphatic flow. Does it destroy ducts, or perhaps physically clog the nodes?
Dear Paul: I covered the topic of infections associated with lymphedema previously – here is the link: https://www.lymphedemablog.com/2010/10/29/infections-associated-with-lymphedema/
Infections caused by filariasis will produce blockage of lymph vessels and nodes. Lymphatic Filariasis will be covered in an upcoming posting.
Dear Mr Zuther and Lymphologists,
An interesting basic article for the beginners. Congratulations!As usually in medicine,which is partly science, partly art based on anecdotal wisdom, there are some traditional views that should be revised once we get objective evidence. This applies among others to the so called high-protein edema. In lymphedema and other type od edema, with exception of acute bacterial or chemical (insect bite), lymph protein concntration is LOW (0.5-3.5g%). Proteins in the interstitial space attract oncotically water from blood capillaries and partly from cells. In effect, the osmotic balance between the capillary lumen and interstitial space is maintained at the cost of increased interstitial space volume (edema). The total mass of protein is increased, however, concentration remains within physiological levels. Starling’s law, with some minor modifications, is still tenable. We published the data on protein concentration in lymph in the 70ties and eighties in journals and books(Lymph stasis- pathomechanism, diagnosis and treatment. CRC Press, Boca Raton, 1991) Could you imagine what would have happened if protein concentration remained high? All tissue cells will become totally dehydrated, as protein will attract the plasmatic and nuclear water. In case of a non-distensible tissue (fibrosis, or non-elastic garment) the interstitial space can not be expanded, tissue fluid pressure increases and capillary filtration stops.This is what we see in elephanthiasis with totally fibrotic tissues. The distensible soft tissues act as a reservoir for flooding fluid. This is different in the stiff skull where brain edema needs fast decompression, otherwise cells die. Compression of limbs increases tissue fluid pressure and water and partly small molecular size protein absorbtion occurs. Proteins pushed to the non-swollen parts of the limb attract water and what we see is swelling of groin and genitals. In course of time they get absorbed. This swelling is a proof of effective compression. Pneumatic compression has been evidently more effective in rapid transfer of edema fluid with proteins than MLD, at least in our studies.
Waldemar L Olszewski
As always, thank you very much for your valued comments, Professor Olszewski!
I sit here in Austria in the Wittlinger Schule for the Dr Vodder method of MLD having just completed successfully the practical exam to practice as a Therapy 1 teacher As I prepare a presentation for the medical team tomorrow, I really enjoyed the detail in the article form a teaching perspective and I thought it was wonderful to see such a swift and relevant response from such a well know name . Thankyou for the time that goes in to putting these articles together and keping us so well informed.
Congratulations on passing your teacher exam!
I am not sure which I have now, in 2006 I was 530+lbs and on oxygen as I had damaged my lungs, my left lower leg swelled to a huge level, I would have fluid seeping out of the skin.
I was sent to a Cardiologist as the 1st EKG showed major heart failure. I asked for a second test as the lady who did the 1st one bruised me badly and I didn’t trust the results, the 2nd EKG done at the Cardiologist office showed no heart issues. He put me on diuretics, I also got a pump machine that inflated booties on both legs as both were effected the left one being way worse.
When he would press on the affected area (from ankle to knee) it would dimple as shown in your picture but he called it lymphedema. I have sense lost the extra weight, regained healthy lungs and work out 6 days a week for 1-3 hrs a day. However my legs (left still the worst) are still swollen no were near as bad and they don’t seep fluid. Most of the skin is loose with occasional flair ups were it gets more swollen. I had had CDT on the left leg and wear 30-40 compression garments on now both legs. Still when it blows up it dimples and never goes below the ankle or above the knee. My skin is soft not hardened so how do I find out what I have? I ask because I would at some point like to have all my extra skin removed, but have been cautioned by my Lymph therapist about that causing worse lymphedema as it would possibly compromise the system even more. I have busted my back side loosing over 300 pounds and do not want to have sagging skin for the rest of my life, but at my age 51 it is doughty full that the skin will recover it’s elasticity after 20-30 years of being stretched to the max.
So I live in Northern Colorado (about an hour from Denver) is there someone you would suggest I speak with about this issue and as to what I really have
Dear Sandy: I would suggest to locate a lymphedema therapist in your area by using the “Find a Therapist” tab on top of this page. The therapist may be able to refer you to a MD knowledgeable in lymphedema.
I have recently learned that kinesio-tape is being used for lymphedema treatments. Can you comment on that please? Also, are there studies done on the effectiveness of this as an adjunctive treatment modality?
Dear Milissa: I would like to refer you to the following webpage: http://www.lymphedemapeople.com/thesite/lymphedema_and_kinesio_taping.htm
Good article – it is always good to reinforce all that I learned in my lymphedema course. It also helps me to explain to my patients what is happening to them.
I am wondering when the medical field – ie: MD’s referring patients, will understand why treatment is necessary before getting a compression garment. I am always getting referrals for sleeves and gloves but nothing about treating the lymphedema. My patients are primarily post-breast surgery and I certainly would think these MD’s would have a better understanding of what these patients need. Many of my patients come to me and have no idea of what they will be doing and are always surprised and overwhelmed by what will be happening to them over the course of treatment. Many of them come to me thinking they are getting a sleeve and glove and that is all. Sadly for me, quite a few of my patients do not follow through with their therapy.
Any suggestions on how I might help my patients to better understand what is happening to them and how important their therapy is?
Carol: Education of the medical field on the proper treatment and management of lymphedema is a main goal of not only this blog and the Academy of Lymphatic Studies, but also many other organizations involved in lymphedema care and research. Patients should refer their physicians to resources like the National Lymphedema Network, the Lymphatic Research Foundation and others in order to educate these individuals on the appropriate and effective treatment modalities for this condition.
Joachim: Would placement of an IV filter (to prevent movement of large clots) in the abdomen be a cause of increased venous pressure and the reason for increased bil leg edema? These filters are placed by cathter in the venous system per my limited knowledge.
Dear Susan: I am not sure about the correct answer and would like to refer your question to someone more knowledgeable.
Do you have any articles or can you give me more info on Lipo-lipedema (If I spelled it correctly) Thank you!
Here is some good information: http://www.lymphedemapeople.com/wiki/doku.php?id=lipedema
I was wondering if there is a website to look up physicians well versed in lymphedema or lymphologist in a specific area. We are in need of a good physician resource regarding lymphedema and unique lymph abnormalities in the upstate NY area?
Dear Kristin: I would suggest to contact the National Lymphedema Network for an updated list of physicians
Hello, I just wanted to thank you for all of the valuable information on your site. Having had lymphedema for 17 years now has made it impossible to do the things I loved. Thanks to people like you, my doctor is now more aware of what types of treatment I need, and the stages to calming my swollen leg. I am proud to announce that there will be a walk held in Texas to help support the research that you all have been doing. Thank you again for your continued support of the Lymphatic Community!
The swelling in my lower left leg, especially the foot came on for no known reason when I was 13-15 years old. Over a 15 year period I would see 9 doctors including three different kinds of specialists who were clueless as to what caused it. The only advice one doctor gave was for me to take a sit down job but he offered no help for the condition. Over the years it became more and more difficult to by shoes. In 2001 a rheumatolgist diagnosed it as “fibromyalgia.” I had none of the classic symptoms of that disorder. In 2004 when I became convinced I in fact had lymphedema and printed out the NLN Position papers on LE diagnosis my primary care physician refused to look at the papers stating I could not not have “lymphedema” because my swelling was non-pitting. He then refused me a referral to a lymphedema specialist, but I went anyway in spite of the fact the insurance did not pay for the visit without a referral. In February of 04, at age 30 I was diagnosed with Primary Lymphedema Type II: Lymphedema Praecox and was reccomended MLD which my insurance would not pay for so I obtained a compression garment. I find it riddiculus it took me 15+ years to get a diagnosis and some relief from this condition due to the lack of education in the medical community. Recently my primary care physician, a new one who cares, informed me that the edema in my foot is now “non-pitting.” I now buy triple wide shoes because of the size of my left foot.
I meant to say my primary care physician in 2004 said it was not lymphedema because the type of swelling I had was pitting.
I recently came across your site and have been reading along. I thought I would leave my first comment. I don’t know what to say except that I have enjoyed reading. Nice blog. I will keep visiting this blog very often.
Susan
After 36 years of lymphedema in both arms resulting from mastectomy of both breasts in 1975, I am still fighting to have blood drawings from right foot, will they ever pass a law for this request to be approved through RED CROSS and ALL HOSPITALS?????? At 90 years old, it seems such a horrible scene to fight for each time the drawing is due>
Hi Joe,
I am a lymphedema therapist. This is a great article! One question I have is how does the body rid debris and other particles that get filtered out through lymph nodes out of the body? Is there a pathway it takes from the lymph nodes to excretion? I, as well as some of my patients, have wondered this multiple times. Any light you can shed on this would be helpful. Thanks!
Julie
Dear Julie: Ultimately, waste products are excreted via the kidneys.
[…] and lymphedema have very different causes and are treated differently. A previous blog post “When is it Lymphedema?” compares these two conditions:Additional […]
Thanks Joe. What’s it’s pathway to the kidneys?
Via the blood
I’m at the beginning of my research on lymphedema and found your article very informative and easy to understand.
Do you know if there’s a connection of lymphedema to thyroid cancer? I’ve had two surgeries that removed lymph nodes (and thyroid, thymus, parathyroids)and I’ve been experiencing swelling. My endo said my lymph nodes are probably not draining.
Thyroid cancer may cause the onset of lymphedema in the head and neck area after removal of the malignant mass and dissection of the lymph nodes in this area.
thanks for this great article! can i to post it on the brazilian blog of lymphedema? thks!
Thank you for this article. I have struggled for a while with controlling my swelling in my legs and through diet, exercise, compression tights and my leg compressor machine – I seem to have it under control. The leg compressor machine is amazing! I do not know what I did without it. It is sad that I will need to monitor this for the rest of my life – and that there is generally no awareness on how severe these conditions can get. I am frequently embarrassed when I have to pass on activities with friends because of swelling. How can you even begin to explain something like this to people who don’t have it and never heard of it?
I have lymphedema and I was wonderning about body wraps that you get at spa’s. Does a body wrap do anything for lymphedema or does it make it worse? I know wraps are designed to make you sweat. Is this a good thing to do?
Dear Priscilla: While these wraps probably do not have negative effects on the swellng since they are applied over a relatively short period of time, we do not recommend these because of the increase in local blood flow, which may negatively effect lymphedema
Thank you for your excellent articles! They are concise, very informative and user friendly.
Great article. There is another, little recognized form of lymphedema called, ‘lymphedema praecox’. My child was diagnosed at twelve after I noticed his foot had swelled with no known external cause of injury. Insurance does not pay for compression garments even though he has been properly diagnosed by a physician and a specialist.
I am going to a Lymphadema clinic and I am going for general swelling throughout my body including abdomen. I recently had Venous Closure for 2 veins in each leg. My Cardiologist thinks once my Vascular system is functioning normal again that everything will return to normal. The Lymphadema clinic says I have to pump 2 hours everyday, be in compression whenever I’m on my feet and do a low sodium diet for the rest of my life. I’m really confused and I’m a Flight Attendant so I can not carry the pump with me. I guess I’m just confused as to whether is Edema or Lymphadema as it’s all over water retention and not isolated to one limb. Thanks!
Lymphedema generally does not manifest itself throughout the body. In the vast majority of the cases only one limb is affected by lymphedematous swelling. Here is a link to an article you may find interesting: https://www.lymphedemablog.com/2011/06/23/when-is-it-lymphedema/
Great article! A coworker and I just presented to our therapy team this exact topic today! I can’t wait to send the team your link. Quick question. When a patient is suffering from CVI why do they usually experience pain on the medial aspect of the ankle and shin? I’m looking more for the physiological answer. I’m having a tough time locating the answer. Thanks for sharing all your valuable knowledge!
Sara: The swelling associated with CVI tends to be painful. Edema is often pronounced in the area of the medial malleolus and it is thought that the pain is caused by the swelling triggering nociceptors in the area.
I suffered for about 4 years with adema not only in my legs but in different parts of my body. It became worse when I traveled. It was very painful and my husband thought I was rediculous when I said I could feel it in m6 neck. About a year later I had a sudden unexpected bowel obsrtuction caused from Adhesions. After the adhesions were removed and mt body healed the adema was never as bad again. I do get swollen ankles but nithing like before. I think my bowel had already beibstructed and was causing the priblem . It just took time for the bowel to be completely closed off.
Thanks for an informative article. My legs started swellIng about 2 years ago and it’s been a couple of months since I was diagnosed with lymphedema and I’ve been receiving respective treatment.After reading this article I was wondering whether something else might be the cause of swelling rather than lymphedema. The case is that I’ve been vegeterian for 4 years now and maybe this caused change in the concentration of serum proteins which lead to edema. This possibility was somehow overlooked by my doctor and now I’m considering a serum protein test just to be sure that it’s lymphedema and not something else. Do you think that this is a possibility?(swelling is contained to my legs only and not the whole body)
Thanks,
Ana – protein in the diet has no effect whatsoever on lymphedema. Here is a link to an article on that subject:https://www.lymphedemablog.com/2010/12/10/nutritional-aspects-in-lymphedema/
Thank you for an interesting and useful article. I have linked to your blog from my website as well as from my Facebook page.
Good article but I am wondering why dont also mention the new and emerging field of microsurgery to address lymphedema. This area is showing great promise in treating the disease especially if done early in an early stage of lymphedema, i have seocondary lymphedema in my left leg due to cancer surgery. I had VLNT – vascularized lymph nide transfer surgery performed this spring and am seeing a significant improvement in my swelling and inflamation on the affected limb. I am so glad I had this procedure done and I wish more people knew about this option.
Dear Patricia: Thank you for your comment – you are correct, microsurgical procedures have come along way and patients who qualify can certainly benefit from these procedures. I will dedicate one of the future articles on this site to this issue.
I have lymphedema and wondered what are the best shoes to get for this condition?
There are no special shoes designed for lymphedema patients. The best options include adjustable brands.
Thank you for your interesting articles, Mr. Zuther!
I’ve noticed parts of my body that feel like they’re getting swollen. It makes sense that this could be my lymph nodes filling up. It would be a good idea for me to find a specialist to help me out with this. They would be able to figure out exactly what’s going on.