
 Joachim Zuther, Lymphedema Specialist.
Joachim Zuther, Lymphedema Specialist.
 Chronic lymphedema is considered to be a progressive condition, regardless of its classification of either primary or secondary, and cannot simply be described as an accumulation of protein-rich fluid. It is a chronic, degenerative and inflammatory process affecting the soft tissues, skin, lymph vessels and nodes of the extremities, trunk, abdomen, head and neck, and exterior genitalia. Lymphedema can develop anytime during the course of a lifetime in primary cases, in secondary cases it may occur immediately following the surgical procedure or trauma, within a few months, a couple of years, or twenty years or more after treatment, and may result in severe and often disabling swelling.
Chronic lymphedema is considered to be a progressive condition, regardless of its classification of either primary or secondary, and cannot simply be described as an accumulation of protein-rich fluid. It is a chronic, degenerative and inflammatory process affecting the soft tissues, skin, lymph vessels and nodes of the extremities, trunk, abdomen, head and neck, and exterior genitalia. Lymphedema can develop anytime during the course of a lifetime in primary cases, in secondary cases it may occur immediately following the surgical procedure or trauma, within a few months, a couple of years, or twenty years or more after treatment, and may result in severe and often disabling swelling.
It is well known and confirmed by research for quite some time 1,2,3,11 that chronic lymphedema considerably impacts the health-related quality of life (QoL) and psychological well-being of patients around the globe affected by this disease.
The highest incidence of secondary lymphedema in the United States is observed following surgery and radiation for malignancies, particularly among those individuals affected by breast cancer, which is conceivably the reason why the majority of research on the impact of lymphedema on QoL was conducted on survivors of breast cancer with subsequent lymphedema (breast cancer related lymphedema/BCRL). The results of this research clearly indicate that health related QoL was significantly lower in breast cancer survivors with diagnosed lymphedema or with arm symptoms without diagnosed lymphedema, compared with survivors without lymphedema or arm symptoms4.
Any woman treated for breast cancer has a risk of developing lymphedema during or after the surgical/radiation/chemotherapy treatment necessary to eradicate the tumor. The impact of these procedures on the sufficiency of the lymphatic system may result in the onset of more or less lymphatic swelling in almost one woman in two.
However, the literature also shows that the QoL of individuals affected by primary lymphedema and other forms of secondary lymphedema is negatively affected as well by this chronic condition. In fact, several studies indicate that patients affected by chronic edema of the lower extremities reported a higher impact on QoL than individuals with upper extremity lymphedema 5 6,7. It is also important to point out that the negative effects on QoL of lymphedema in many cases extends to the families of those living and coping with chronic edema 8,9.
 As soon as, and sometimes before the swelling manifests itself, patients are confronted by esthetic problems (skin changes, increase in extremity size, ill-fitting clothing), functional problems (pain, stiffness, numbness, functional limitations, limitations in range of motion in the affected extremity, compromised normal activities of daily living and occupational responsibilities), psychological problems (negative self-identity, emotional disturbance, stress, negative impact on family life, social isolation, perceived reduced sexuality), as well as financial impact. When some patients realize that lymphedema is a chronic disease requiring life-long management, these problems may intensify, and patients feel that coping with the swelling is more demanding than the treatment of the disease that caused lymphedema in the first place.
As soon as, and sometimes before the swelling manifests itself, patients are confronted by esthetic problems (skin changes, increase in extremity size, ill-fitting clothing), functional problems (pain, stiffness, numbness, functional limitations, limitations in range of motion in the affected extremity, compromised normal activities of daily living and occupational responsibilities), psychological problems (negative self-identity, emotional disturbance, stress, negative impact on family life, social isolation, perceived reduced sexuality), as well as financial impact. When some patients realize that lymphedema is a chronic disease requiring life-long management, these problems may intensify, and patients feel that coping with the swelling is more demanding than the treatment of the disease that caused lymphedema in the first place.
In order to effectively combat not only the swelling, but also the negative impact of lymphedema on psychological well-being, early diagnosis, evaluation and coordinated multi-disciplinary treatment strategies by certified lymphedema therapists and qualified health care professionals are imperative.
By definition, the goal of all treatment is to improve the patient’s state of health; addressing the quality-of-life consequences of the patient has an important role to play alongside the objective of reducing limb volume.
Studies indicate that QoL improves with reduction in limb volume10; early diagnosis and subsequent efficient therapeutic intervention for lymphedema is therefore crucial to optimal 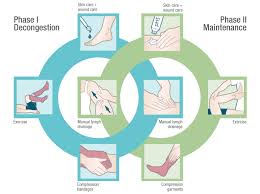 treatment outcomes. However, effective lymphedema management should not only include comprehensive treatment measures by qualified health care providers to reduce the swelling, combined with education of the patients in regard to self-care measures; it should also address the QoL consequences of the disease and improve health related QoL and psychological well-being by evaluating psychological and psychosocial criteria, and educating the patient on social support groups and interactive support.
treatment outcomes. However, effective lymphedema management should not only include comprehensive treatment measures by qualified health care providers to reduce the swelling, combined with education of the patients in regard to self-care measures; it should also address the QoL consequences of the disease and improve health related QoL and psychological well-being by evaluating psychological and psychosocial criteria, and educating the patient on social support groups and interactive support.
In addition to treating the lymphatic swelling, the lymphedema therapist plays an important role in educating the patient in regard to the treatment measures and self-care techniques (self-MLD, self-bandaging, skin and nail care, etc.). Oftentimes patients have a hard time accepting  the need for the application of bulky padded compression bandages on the affected extremity during the intensive phase (phase 1) of Complete Decongestive Therapy; compression bandages are necessary to address the fluctuating volume of the lymphedema during this intensive phase, in which the patient is treated ideally on a daily basis. In order to reduce anxiety and improve patient compliance, it is crucial for the patient to know, that the need for compression bandages is only temporary. Once the swollen body part is decongested and the patient transitions into phase 2 of CDT (self-management phase), the bandages will be replaced by fitted compression garments.
the need for the application of bulky padded compression bandages on the affected extremity during the intensive phase (phase 1) of Complete Decongestive Therapy; compression bandages are necessary to address the fluctuating volume of the lymphedema during this intensive phase, in which the patient is treated ideally on a daily basis. In order to reduce anxiety and improve patient compliance, it is crucial for the patient to know, that the need for compression bandages is only temporary. Once the swollen body part is decongested and the patient transitions into phase 2 of CDT (self-management phase), the bandages will be replaced by fitted compression garments.
Dear Lymphedema Blog Reader – if you like the contents on this website, please help to keep it going. A great amount of work and research is necessary to provide you with up-to-date information on this site. Your donation supports these efforts and associated administrative costs. Surplus funds will be donated to Lymphedema/Lipedema-related charitable endeavors. Please donate using the “Donate Now” button on the right upper hand of this page – Thank You!
Do you need more information on other topics on lymphedema? Use the “Index” list on the left side of this page and select the article you are interested in. You can also use the “Select Category” window on the right of this page and select the topic you are interested in. Once selected, a new page will load with a number of articles related to the topic you chose. Click on any headline of the articles and the entire article will load up for you to read.
Join Lymphedema Guru, a Facebook page solely dedicated to inform about all things related to lymphedema – news, support groups, treatment centers, and much more
References:
- Fu M, Ridner SH, Hu SH, Cormier JC, Armer JM. Psychosocial impact of lymphedema: a systematic review of literature (2004–2011). Psycho-Oncology 2013; 22(7):1466-1484
- McWayne J, Heiney SP. Psychologic and social sequelae of secondary lymphedema: a review.
Cancer 2005;104(3):457–466 - Ridner SH et al. Breast cancer treatment related lymphedema self-care; eduction, practices symptoms, and quality of life. Suppoort Care Cancer, 2011; 19(5):631-637
- R.Ahmed et al. Lymphedema and Quality of Life in Breast Cancer Survivors: The Iowa Women’s Health Study. J Clin Oncol. 2008 Dec 10; 26(35): 5689–5696. Published online 2008 Nov 10. doi: 10.1200/JCO.2008.16.4731
- Greene A, Meskell P. The impact of lower limb chronic oedema on patients’ quality of life. Int Wound J 2017; 14:561–568.
- Moffatt CJ, Aubeeluck A, Franks PJ, Doherty D, Mortimer P, Quere I. Psychological factors in chronic oedema: A case-control study. Lymphat Res Biol 2017; 15:252–260.
- Moffatt CJ, Doherty DC, Franks PJ, Mortimer PS. Community based treatment for chronic edema: An effective service model. Lymphat Res Biol 2018; 16:92–99.
- Radina ME, Armer JM. Post-breast cancer lymphedema and the family: A qualitative investigation of families coping with chronic illness. J Fam Nurs 2001;7(3):281–299.
- Radina ME, Armer JM. Surviving breast cancer and living with lymphedema: resiliency among women in the context of their families. J Fam Nurs 2004;10(4):485–505
- Mirolo BR, Bunce IH, Chapman M, et al: Psychosocial benefits of postmastectomy lymphedema therapy. Cancer Nurs 18:197-205, 1995
- Zuther, J, Norton, S. Lymphedema Management: The Comprehensive Guide for Practitioners. 4th ed. New York: Thieme; 2018.


[…] READ THE ARTICLE FROM LYMPHEDEMA BLOG. […]
Am 42 been living with lymphedema for 10 yrs now in both my legs at first my Dr didn’t know what it was so he kept putting me on water pills and it didn’t help so it got worse every doctor I went to didn’t know anything about lymphedema til I research it and diagnosed my self with it and finally had a ultra sound done showing my valves in my upper thigh area were damaged and instead of pumping fluid in and out like it should it was just staying opened I seen the top vascular surgeon at UCSF n he basically told me I had to live like this for the rest of my life hearing that was devastating I went into full blown bipolar depression tried to kill my self numerous times but am still hear asking and screaming for help from different vein clinics on what type of surgeries can be done to help me and still nothing so I basically have to lay in bed all day with my legs elevated to keep the swelling down I used to have the lymph press but was taken from me when I lost everything when I lost my home