
 Joachim Zuther, Lymphedema Specialist.
Joachim Zuther, Lymphedema Specialist.
The swelling in lymphedema is caused by an abnormal accumulation of protein and water molecules in the tissue, and results from the inability of the lymphatic system to perform one of its basic functions, the removal of water and protein from the body tissues. In primary lymphedema, this insufficiency is caused by developmental abnormalities of the lymphatic system; damage to the lymphatic system, such as the removal or radiation of lymph nodes in cancer surgery, or infection of the lymphatic system are causes of secondary lymphedema.
Lymphedema is a common and serious condition affecting at least 3 million Americans; the highest incidence of secondary lymphedema in the United States is observed following surgery and radiation for malignancies, particularly among those individuals affected by breast cancer. At the present time, almost 280,000 new cases of breast cancer in females and 2700 in males are diagnosed in the United States annually (1). Primary lymphedema is far less common than the secondary form; it has been estimated to affect 1 in 100,000 people worldwide (2), most commonly female patients with a ratio of one male to three females. In most cases of primary lymphedema cases, the lower extremities are affected.
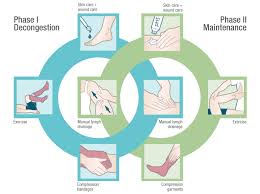
Components and Phases of Complete Decongestive Therapy (CDT)
The internationally recognized gold standard treatment for lymphedema is Complete Decongestive Therapy (CDT). CDT is performed in two phases; in phase one, also known as the intensive or decongestive phase, treatments are administered by appropriately trained and certified lymphedema therapists, ideally on a daily basis, until the affected body part is decongested.
The end of the first phase of CDT is determined by the results of measurements on the affected body part, which are taken by the therapist. Once measurements approach a plateau, the end of phase one is reached and the patient progresses seamlessly into phase two of CDT, also known as the self-management phase. Phase two is an ongoing and individualized part of CDT, in which the patient assumes responsibility for maintaining and improving the treatment results achieved in phase one.
CDT lymphedema training consists of a minimum of 135 hours of instruction, comprised of 1/3 theoretical (45 hours), and 2/3 live practical (90 hours) in-person instruction format. The credential of Certified Lymphedema Therapist (CLT) is earned upon successful completion of a training course.
The current state of training for Certified Lymphedema Therapists (CLT’s) is at the highest proficiency standard in history, whereby it is understood that live hands-on training in schools specialized in the training and certification of CLT’s remains the only effective and responsible system for developing the necessary manual skills to treat a disease as complex as lymphedema. This has been proven for nearly 30 years via live instructor assessment and the honing of skills in a classroom of peers, similar to all other rehabilitation, medical, and surgical training programs.
As previously announced, the Lymphology Association of North America (LANA®), an organization offering accredited certification examinations to healthcare specialists treating lymphedema, changed their eligibility requirements to sit for the LANA® exam effective January of 2022. The new requirements allow the entire 135-hour certification course for CLT’s to be taught virtually, without certified instructors being physically present during instruction, including the hands-on practical lab work.
Let that sink in………..a highly specialized medical manual treatment technique that is learned remotely!
Would you want to have your baby delivered by a remotely instructed midwife, or have your teeth cleaned by a dental hygienist, who learned the technique online?
Remote learning has its strengths, however, hands-on, practical instruction in the treatment and management of a condition as prevalent and serious as lymphedema, is most certainly not one of these techniques that can be taught remotely (neither asynchronous nor synchronous remote).
As a lymphedema specialist with almost 40 years of experience in both the treatment of patients suffering from lymphedema and the training of thousands of CLTs, I can assure the readers that the manual techniques used in the treatment of lymphedema are highly specialized and cannot be compared to any other techniques a therapist has learned and practiced in their earlier education and patient interaction. A live practical directive from certified instructors and feedback from student peers on tactile input is essential in building hands-on skills for lymphedema therapists.
Unfortunately, LANA’s decision to change the training requirements for Certified Lymphedema Therapists to allow the entire 135-hour certification course to be taught virtually, without certified instructors being physically present, including the hands-on practical lab work (!), has led to the development of lymphedema training schools offering virtual, or hybrid Lymphedema certification courses; this will inevitably prove to move the bar for responsible training for CLT’s to an all-time low.
Responsible CDT schools, such as the Norton School of Lymphatic Therapy, have resisted this new model and continue to offer quality lymphedema certification; live hands-on training in schools specialized in the training and certification of CLTs remains the only effective and responsible system for developing the necessary manual skills to treat this disease.
Patients suffering from lymphedema should make sure that their therapist learned the hands-on treatment techniques in a live classroom setting!
References
- US Breast Cancer Statistics. Retrieved from www.breastcancer.org/facts-statistics (accessed May 2022)
- Arin K. Greene, Jeremy A. Goss Diagnosis and Staging of Lymphedema Semin Plast Surg. 2018 Feb; 32(1): 12–16. Published online 2018 Apr 9. doi: 10.1055/s-0038-1635117 PMCID: PMC5891654
Dear Lymphedema Blog Reader – if you like the contents on this website, please help to keep it going. A great amount of work and research is necessary to provide you with up-to-date information on this site. Your donation supports these efforts and associated administrative costs. Surplus funds will be donated to Lymphedema/Lipedema-related charitable endeavors. Please donate using the “Donate Now” button on the right upper hand of this page – Thank You!
Join Lymphedema Guru, a Facebook page solely dedicated to informing about all things related to lymphedema – news, support groups, treatment centers, and much more


Thank you for continuing to expose this dreadful decision by LANA. As a CLT, I have personally written to LANA more than once, obviously to no avail. It is indeed unthinkable that effective therapists could be trained virtually in a hands-on modality. I recently took a short virtual classes that promised certification to see for myself. It was worse than I’d imagined.
So disappointing to learn that an intimate effective tactile modality and the required proficiency to perform it effectively is being considered superfluous in the view of bureaucratic individuals. They seem to value the acquisition of pseudo skills thus depriving patients seeking relevant treatment, of the benefits of receiving the services only a skilled practitioner can provide. Who stands to benefit? Certainly not our patients.
Thanks for being the voice of integrity. I can never understand how a manual worker can get full concept of what they learned without getting to experience how it affects their own body from treatment in classroom exchanging with their classmates. I think they feel they can get away with it from desparate measure of online training during pandemic lockdown. However, there are so many studies shown that children who went through online learning, even when it’s not manual study, lose the grasp of subject without benefit of interaction in personal level. It’s like allowing surgeon who never had hands-on learning experiences to operate on you, though not as acutely effecting health of the patients but I for one would not want to be a Guinea pig for someone to take the cost-saving ways to learn