
 Joachim Zuther, Lymphedema Specialist.
Joachim Zuther, Lymphedema Specialist.
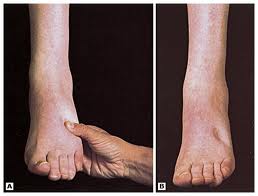
Pitting
Lymphedema is a very common and serious condition, affecting at least 3 million Americans. However, there is no consistency, as well as a lack of literature regarding the data on the general incidence of primary and secondary lymphedema. Incidence rates in the literature vary greatly, which results from the variety of measurement techniques and definitions used in studies that evaluate the rates of lymphedema. The true numbers of patients affected by any form of lymphedema are unknown.
Other than skin cancer, breast cancer is the most common type of cancer among women in the United States. All women are at a lifetime risk for developing breast cancer and a woman’s chance of developing breast cancer increases with age. The incidence of breast cancer treatment related lymphedema (BCRL) is generally poorly documented due to delayed onset of symptoms and the lack of standardized diagnostic criteria. Up to 40 percent of the 3 million cancer survivors in the United States will develop breast cancer treatment related lymphedema 1,2. It is generally thought that the more lymph nodes are removed during any surgical procedure, the higher the incidence of lymphedema.
Other cancer survivors at risk for lymphedema include those who have undergone surgery and/or radiation treatment for malignant melanoma, prostate cancer, gynecologic cancers, ovarian and testicular cancers, and colorectal, pancreatic, or liver cancers.
The incidence of secondary lower extremity lymphedema is even less well documented than that for secondary upper extremity lymphedema. Lymph node dissection for malignant melanoma has been shown to have an incidence risk of lymphedema of up to 80 percent, though other studies suggest an incidence between 6 to 29 percent 3. Treatment for cervical, endometrial, and vulvar malignancies has been shown to have an incident risk of lymphedema between 5 and 49 percent; incidence rates increase if treatment involves radiation therapy 3. In prostate cancer, the incidence of lymphedema has been observed at 3 to 8 percent, which has been shown to increase with the use of radiation therapy by three to fourfold 3.
Regular and early screening for lymphedema is frequently recommended in the literature. Evidence indicates that early detection of latent lymphedema offers an opportunity to identify and treat lymphedema more successfully at an earlier stage, when lymphedematous components are still in the fluid stage and reversible, in order to avoid progression into an “irreversible” stage. This is also addressed in the National Lymphedema Network’s (NLN) Position Paper on “Screening and Measurements for Early Detection of Breast Cancer Related Lymphedema” 4.
Researchers and clinicians have used multiple methods of screening for lymphedema and evaluating limb volume, and opinions vary regarding the most effective and accurate measurement technique. These methods include water displacement, circumferential measurement with a tape measure (with or without limb volume calculation using computer software), infrared scanning (perometry), and bioelectrical impedance spectroscopy. Currently, new portable infrared 3-D scanners are field tested (6). Other imaging techniques used for both diagnostic and evaluation purposes include Magnetic Resonance Imaging (MRI) and Computed Tomography (CT). These techniques are costly and require equipment generally not available in lymphedema treatment centers.
It is important to point out that regardless of what method is used, that the method is consistent (different methods are not interchangeable), the measurement protocols are standardized and be taken by the same individual on the same patient during the entire assessment phase.
Effective screening for lymphedema not only increases treatment outcomes, but also potentially helps to reduce lymphedema treatment-related costs. Stout et.al pointed out that a prospective surveillance model for breast cancer treatment related lymphedema (BCRL) can serve as a potential cost-saving mechanism for BCRL treatment 5. In this comparison, the projected per year cost of a prospective screening model for lymphedema was considerably lower than the cost for traditional management of lymphedema ($636.19 vs. $3124.92 using 2009 Medicare rates).
Most Common Screening Methods used for the Detection of Lymphedema
The need to prospectively screen patients for the development of lymphedema is well understood. Early detection of lymphedema is imperative for early intervention and prevention of chronic lymphedema. The patients play an important role in this process and should be educated regarding signs and symptoms of developing lymphedema, such as perceived swelling and the sensation of heaviness, tightness and to report any of these signs immediately to their health care provider.
Each of the below listed screening and measurement methods are valid for assessment of limb lymphedema. When deciding which technique to use, health care providers may want to consider issues such as the time required to conduct the measurements, cost of equipment, and the potential for user error.
Water Displacement
 The water displacement method is regarded as the gold standard for measuring limb volume and is the only reliable method available to assess edema of the hands and feet. This method follows Archimedes’ Principle that an object immersed wholly or partially in fluid will displace its own volume of water. This technique uses volumeters filled with water and equipped with an overflow spout and a beaker. The extremity is then partially or completely immersed in the water, and the displaced water is collected in the beaker. The amount of displaced water represents the extremity volume. This method, although highly accurate, is limited by hygiene issues and cannot be used with patients having open wounds or sores. In addition, the water displacement method is cumbersome and requires the removal of clothing covering the limb.
The water displacement method is regarded as the gold standard for measuring limb volume and is the only reliable method available to assess edema of the hands and feet. This method follows Archimedes’ Principle that an object immersed wholly or partially in fluid will displace its own volume of water. This technique uses volumeters filled with water and equipped with an overflow spout and a beaker. The extremity is then partially or completely immersed in the water, and the displaced water is collected in the beaker. The amount of displaced water represents the extremity volume. This method, although highly accurate, is limited by hygiene issues and cannot be used with patients having open wounds or sores. In addition, the water displacement method is cumbersome and requires the removal of clothing covering the limb.
Circumferential Measurements
 Circumferential measurements are taken at various intervals of the limb in order to calculate volume. Measurements are taken at the same exact points on the individual each time; it is therefore necessary to document each measurement point in the patient’s chart. Although portable and inexpensive in regard to equipment cost, this frequently used method is time intensive, requires extensive experience by the clinician, and patients must remove clothing from the limb as they do with water displacement. There are also some concerns regarding the reliability of the measurements. Clinicians measuring extremities with a tape measure may hold the tape either tightly or loosely around the limb, causing variation in circumferential measurements. This may cause considerable measurement errors when calculating volume, which can potentially mask lymphedema progression, or falsely imply lymphedema. A spring-loaded measuring tape may be more suitable to take measurements, especially if more than one clinician is involved in the measurements. Limitations for the use of this method also include skin damage.
Circumferential measurements are taken at various intervals of the limb in order to calculate volume. Measurements are taken at the same exact points on the individual each time; it is therefore necessary to document each measurement point in the patient’s chart. Although portable and inexpensive in regard to equipment cost, this frequently used method is time intensive, requires extensive experience by the clinician, and patients must remove clothing from the limb as they do with water displacement. There are also some concerns regarding the reliability of the measurements. Clinicians measuring extremities with a tape measure may hold the tape either tightly or loosely around the limb, causing variation in circumferential measurements. This may cause considerable measurement errors when calculating volume, which can potentially mask lymphedema progression, or falsely imply lymphedema. A spring-loaded measuring tape may be more suitable to take measurements, especially if more than one clinician is involved in the measurements. Limitations for the use of this method also include skin damage.
Infrared Perometry

Perometer
This method, although expensive, provides more reliable results than the circumferential tape measurement technique and was developed to provide a quick, hygienic method of determining limb volume. The affected extremity is inserted into a vertically or horizontally orientated frame that emits two parallel arrays of infrared light beams at right angles to each other. The limb casts shadows that are observed by receivers on the opposite two sides of the frame to the light emitters, and two transverse diameters of a portion of the extremity are measured. The Perometer frame is moved along the extremity, allowing measurements to be taken every 3 millimeters (mm). Operation with a conventional computer allows simple monitoring and makes accurate calculations of changes in volume of any part of the extremity in a matter of seconds.
The equipment itself does not touch the skin, allowing measurements to be taken on extremities with sensitive or broken skin. However, it is difficult to obtain accurate measurements in individuals who cannot maintain a stable position during measurement, and it is difficult to measure the most proximal part of the upper arm or thigh.
Bioelectrical Impedance Analysis
This technique is also known as bioimpedance analysis (BIA), or bioimpedance spectroscopy (BIS) was first used over 30 years ago to measure the total water content of the body. More recently, however, BIA has been used for the quantification of unilateral and bilateral limb extracellular fluid. BIA involves passing a very small electrical current through the body tissues, which is then used to determine the electrical impedance (or opposition) to the flow of the electric current through body tissues. This value is then used to determine extracellular fluid volume and provides the difference in fluid between the affected and non-affected limb.

This technique carries a low risk of user error and is easy to use.
Dear Lymphedema Blog Reader – if you like the contents on this website, please help to keep it going. A great amount of work and research is necessary to provide you with up-to-date information on this site. Your donation supports these efforts and associated administrative costs. Surplus funds will be donated to Lymphedema/Lipedema-related charitable endeavors. Please donate using the “Donate Now” button on the right upper hand of this page – Thank You!
Join Lymphedema Guru, a Facebook page solely dedicated to informing about all things related to lymphedema – news, support groups, treatment centers, and much more.
- Ostby PL, Armer JM. Complexities of Adherence and Post-Cancer Lymphedema Management. J.Pers. Med. 2015, 5, 370-388; doi:10.3390/jpm5040370. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4695861/
- Norman SA, Localio AR, Potashnik SL, et al. Lymphedema in breast cancer survivors: incidence, degree, time course, treatment, and symptoms. J Clin Oncol 2009;27(3):390-397 PMID:19064976. Available online: https://www.ncbi.nlm.nih.gov/pubmed/19064976
- Rockson SG, Rivera KK. Estimating the population burden of lymphedema. [Review][109 refs]. Ann NY Acad Science 2008; 1131: 147-154. PMID 18519968
- National Lymphedema Network National lymphedema network supplement to the national lymphedema network position statement breast cancer screening: Screening and early detection of breast cancer-related lymphedema. Available online: https://www.lymphnet.org/pdfDocs/nlnBCLE.pdf
- Breast cancer-related lymphedema: comparing direct costs of a prospective surveillance model and a traditional model of care. Stout NL, Pfalzer LA, Springer B, Levy E, McGarvey CL, Danoff JV, Gerber LH, Soballe PWPhys Ther. 2012 Jan; 92(1):152-63. Available online: https://www.ncbi.nlm.nih.gov/pubmed/21921254
- https://ajtmh.org/content/journals/10.4269/ajtmh.17-0504,
http://genetics.wustl.edu/2017/10/16/portable-3-d-scanner-assesses-patients-with-elephantiasis/


What info do you have about Lipedema (different condition from lymphedema)
Thank you
There are a number of articles on lipedema on this page. Just click on any article link you may be interested in on the “index” list to the left.
Very good information. Thank you. Hope you continue sending information from time to time.
Very helpful post! thanks for sharing!